
NETSPOT (68Ga-Dotatate) is a radioactive diagnostic agent used for PET imaging that is gaining ground among practices.
FDA-approved in 2016, NETSPOT is used in imaging to locate somatostatin receptor positive neuroendocrine tumors in adult and pediatric patients. The commercial product is a single dose kit for the preparation of a 68Ga-Dotatate injection manufactured by Advanced Accelerator Applications of Saint Genis-Pouilly, France.
For PET imaging facilities who may be more used to using Octreotide or Octreoscan, NETSPOT may prove to be a good alternative. Here, we aim to answer a few key questions about NETSPOT and how it is used:
Background on NETSPOT
Neuroendocrine tumors are malignant and benign tumors that affect an estimated 47,300 individuals in Europe and the United States each year. The tumors develop in the hormone-producing cells of the body’s neuroendocrine system, and are located in organs such as the stomach, intestines, pancreas, and lungs.
Neuroendocrine tumors have receptors for somatostatin, a hormone that regulates the endocrine system. 68Ga-Dotatate, a positron-emitting analog of somatostatin, works by binding to such receptors. The uptake of 68Ga-Dotatate reflects the level of somatostatin receptor density in neuroendocrine tumors.
Until recently, providers relied heavily on the results of Octreotide (or Octreoscan) and MIBG scans for treatment guidance for somatostatin receptor-positive neuroendocrine tumors (NETs). The Octreotide and MIBG imaging often left referring physicians with unanswered questions while having the patient undergo multiple days of imaging and uncomfortable prep.
For example, here is the description of patient preparation a review published in the International Journal of Endocrinology Oncology:
“Long acting octreotide should be discontinued 4 to 6 weeks prior to imaging and the patient should be transitioned to a short acting regimen. For OctreoScan, patients need only to void prior to image acquisition. Though if the abdomen is the area of interest, use of an over-the-counter laxative the night prior to imaging may minimize the amount of nonpathologic uptake in the bowel, as approximately 2% of the labeled somatostatin analog is cleared via the hepatobiliary system and will end up in the intestine.”
They describe OctreoScan as having “moderate sensitivity” as a stand-alone study and limitations in terms of tumor size. It usually has to be used with SPECT and CT.
With NETSPOT (68Ga-Dotatate), the imaging process is completed within a few hours, does not involve any major prep and provides more definitive results than Octreotide. The results from the completed examinations also provide clinicians with information that is quantitative and qualitative, which allows for improved lesion monitoring.
As demonstrated by the data below (1), NETSPOT is the clear choice for providers and patients with NETs.
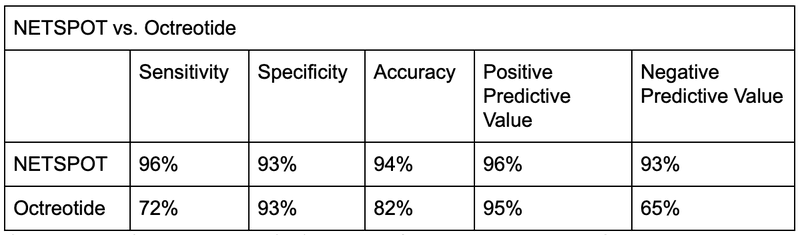
Compared to Octreotide, NETSPOT is 33.3% more sensitive, 14.6% more accurate, yields a 1.1% higher PPV and a 43.1% NPV.
NETSPOT (68Ga-Dotatate), an approved PET/CT imaging agent, is used for the localization of somatostatin receptor-positive neuroendocrine tumors (NETs) in adult and pediatric patients (2).
Clinical outcomes
NETSPOT provides a significant improvement over traditional diagnostic tools. This PET imaging agent provides improved sensitivity and accuracy in addition to providing 100 times more affinity for somatostatin receptors than Octreoscan. This equates to vastly improved imaging that helps clinicians detect 30% more lesions than Octreoscan, resulting in 71% of patients undergoing a change in their disease management. The result is fewer futile surgeries and improved predictive ability to determine response to somatostatin receptor-mediated therapies, including PRRT4.
[ Content upgrade with ID = 1453 not found ]A review of three separate patient case studies found that the improved sensitivity uncovered a larger disease burden. It can have a vital role to play in the decision to alter current treatment where further lesions are identified.
Additionally, NETSPOT allows patients to experience lower doses of radiation with a lower effective dose and higher typical injected activity compared to Octreoscan, which can be 3 to 5 times higher (4). The higher patient throughput of NETSPOT also allows clinics to free up their general nuclear medicine cameras for other examinations, resulting in increased revenue for the department.
Patient preparation
The following points are for patient preparation for NETSPOT (5,6):
- The patient should be advised to hydrate well prior to the appointment.
- There is no need for fasting prior to appointment.
- There are no physical or activity restrictions prior to the appointment.
- If the patient is prescribed somatostatin analogs:
- Long-acting – withhold dosing until imaging is complete
- Short-acting – can be used up to 24 hours prior to imaging
Dosage and administration
The recommended dosage is calculated by patients’ weight. 0.054 mCi/kg should be administered, up to a maximum of 5.4 mCi. For most adult patients, the dosage administered will be 5.4 mCi 68Ga-Dotatate.
Test procedure
Prior to administering NETSPOT, it is imperative that the staff measures the dose to be administered, following the weight-based calculation. The radiopharmaceutical is administered intravenously and should be flushed with normal saline to ensure delivery of the dose in its entirety. Once administered, the IV is no longer necessary and may be removed.
Imaging should begin between 40 and 90 minutes post-intravenous administration of 68Ga-Dotatate. It is recommended to have the patient void prior to imaging. The scan range for NETSPOT imaging is a whole-body acquisition from the top of the skull to mid-thigh. Ideally, the imaging is performed with the patient in the supine position on the PET/CT system with their arms raised above their head. If the patient is unable to comfortably raise their arms, it is recommended to secure them in a resting position at the sides of the body. Standard PET/CT exam protocols may be used for imaging.
Image reconstruction
There is no standard requirement for image reconstruction. It is recommended to reconstruct the PET/CT images following the standard methods set forth by the imaging facility.
Interpretation
Interpretation for PET/CT examinations using NETSPOT is different than standard FDG PET/CT imaging. NETSPOT specific training is available and is recommended for every interpreting physician. 68Ga-Dotatate binds to somatostatin receptors. Based upon the intensity of the signals, PET images obtained using 68Ga-Dotatate indicate the presence and density of somatostatin receptors in tissues. Tumors that do not bear somatostatin receptors will not be visualized. Increased uptake in tumors is not specific for NETs6.
Limitations
A review in Pancreas notes the following limitations:
- 68Ga-DOTATATE PET/CT for surveillance after resection: To date, studies have not directly compared sites of NET disease identified by 68Ga-DOTATATE PET/CT to those identified by cross-sectional imaging in the setting of surveillance after resection. For this reason, there is currently no data to clarify or support a role for 68Ga-DOTATATE PET/CT for surveillance in the adjuvant setting.
- Insurance coverage and reimbursement of costs for patients receiving 68Ga-DOTATATE PET/CT: The FDA-approval of Netspot allows any nuclear medicine facility with PET-CT scanning ability to perform 68Ga-DOTATATE PET/CT imaging. In the United States, 68Ga-DOTATATE PET/CT is not widely available at all nuclear medicine facilities. Furthermore, despite FDA approval and inclusion in the 2017 NCCN guidelines as a diagnostic study, coverage for 68Ga-DOTATATE PET/CT is not routine for all insurance plans. As our use of 68Ga-DOTATATE PET/CT increases for patients with NETs, the financial toxicity of this imaging modality will require review.
Summary
NETSPOT (68Ga-Dotatate) can greatly improve PET imaging accuracy for the localization of somatostatin receptor-positive neuroendocrine tumors (NETs). While it has thus far not been widely available, it is worth looking at if you regularly scan for these indications.
NETSPOT has a clear advantage over other methods with minimal patient preparation and discomfort, and greater sensitivity for detection. It is both FDA and Medicare-approved.
References:
1. Advanced Accelerator Applications. (2017). Overview of NETSPOT [Brochure]. AAA. Retrieved April 15, 2019.
2. Advanced Accelerator Applications. (2017). NETSPOT Reimbursement Kit[Brochure]. AAA. Retrieved April 15, 2019.
3. National Comprehensive Cancer Network. (2019, January). NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines). Neuroendocrine and Adrenal Tumors. Version 1.2019-March 5, 2019. Retrieved April 29, 2019, from https://www.nccn.org/professionals/physician_gls/pdf/neuroendocrine.pdf
4. Advanced Accelerator Applications. (2017). AAA-Ga-68 dotatate NETSPOT_Summary [Brochure]. AAA. Retrieved April 29, 2019.
5. American College of Radiology. (2018). ACR Practice Parameter of the Performance of Gallium-68 Dotatate PET/CT for Neuroendocrine Tumors. Retrieved April 26, 2019, from https://www.acr.org/-/media/ACR/Files/Practice-Parameters/DOTATATE_PET_CT.pdf
6. Advanced Accelerator Applications. (2017). General Gallium Information for Requests [Brochure]. AAA. Retrieved April 29, 2019.
